Neighborhood 2 — Shoulder & Arm
The Assistant Foreman
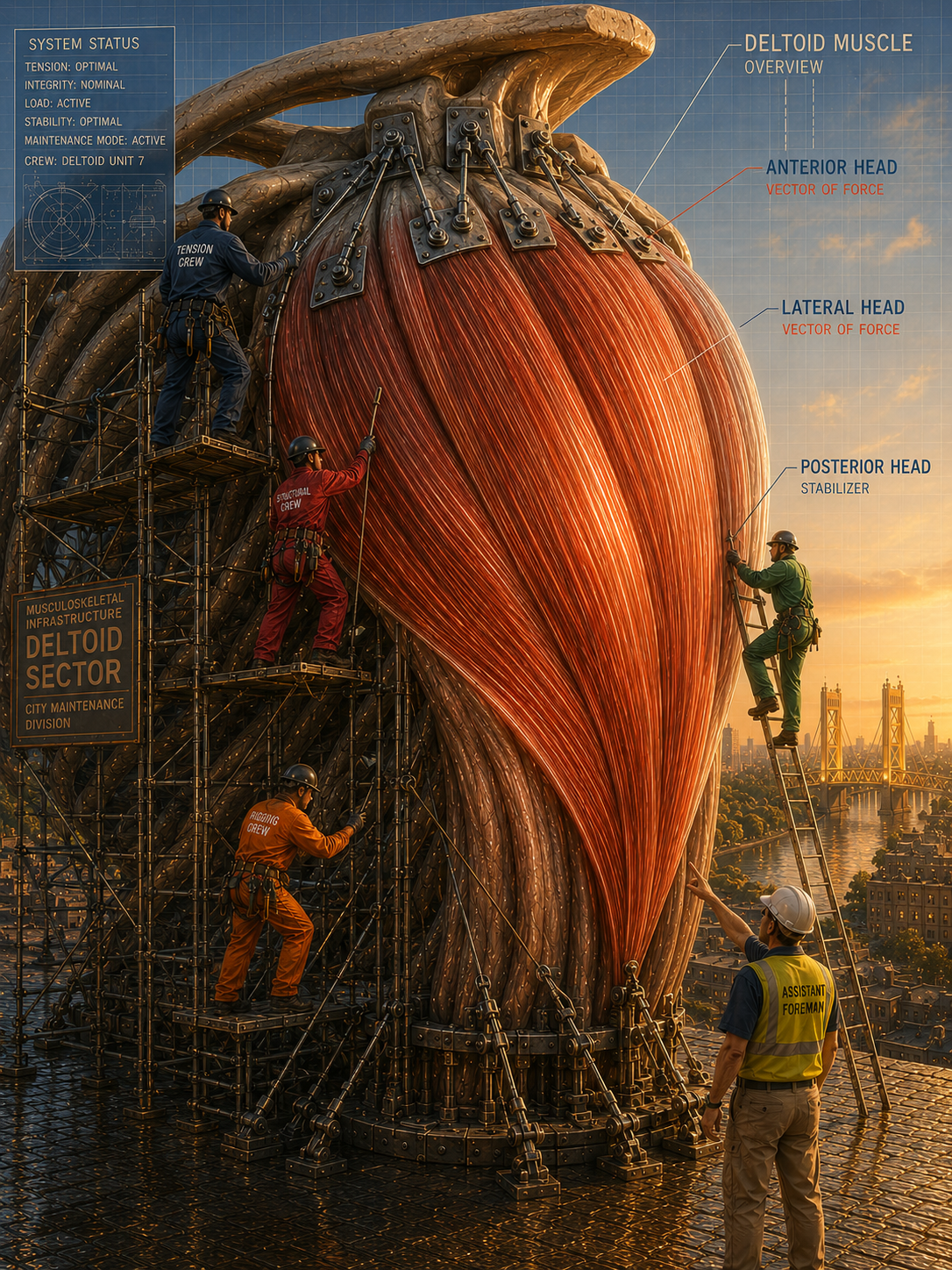
Worker 8 — Deltoid
The deltoid is the muscle people actually see. It’s the curve of the shoulder, the roundness that shows up when someone lifts their arm, the thing that gets credited when a shoulder looks strong. The deltoids do real work. They manage abduction, flexion, extension and all the obvious arm movements that make daily life functional. But the deltoid is an assistant foreman for a reason. It’s not running the operation. It’s executing the plan. And when the people above it stop doing their jobs, the assistant foreman ends up carrying more than his share.
Most people don’t notice their deltoid. Until it starts complaining about a localized ache at the outside of the shoulder, soreness after overhead activity, or fatigue that settles in during repetitive movements that didn’t used to be a problem. What’s less clear is why it started. The deltoid didn’t change. The demand on it did. Something else stopped pulling its weight, and the deltoid picked up the difference without being asked.
The rotator cuff is the most common reason this happens. When the rotator cuff isn’t keeping the humeral head properly centered in the socket, the deltoid has to generate more force to accomplish the same movement. It’s like trying to open a door that’s slightly off its hinges — you can do it, but it takes more effort than it should, and over time that extra effort adds up. The deltoid starts working in ranges and at loads it wasn’t designed to sustain alone. The shoulder still moves. It just costs more than it used to.
The deltoid’s mechanical advantage changes when the shoulder blade isn’t sitting where it belongs. Tilted forward, sitting low, not moving the way it should during arm elevation — the muscle has to work from a position that reduces its efficiency, which means it recruits harder to produce the same output. People feel this as a shoulder that tires quickly, or one that feels unstable at certain angles, or one that aches after activities that never used to register.
“The deltoid is doing its job. It’s just doing everyone else’s job too.”
Pitchers, swimmers, or people who spend a lot of their workday reaching above the shoulder — these people whose deltoids are already operating at a high volume understand this dynamic more than most. When rotator cuff fatigue, poor scapular mechanics, or a tight pectoralis minor shifts the load further onto the deltoid, the margin for error disappears fast. The shoulder that was managing fine starts to send signals. At first those signals are easy to ignore. Eventually they aren’t.
What the pain feels like depends on where in the deltoid the load is concentrated. Anterior deltoid issues tend to show up with forward flexion and internal rotation, like reaching across the body or lifting something from a low shelf in front of you. Lateral deltoid complaints are usually tied to abduction, the straight-out-to-the-side movement that puts the most demand on the muscle. Posterior deltoid problems are less common but tend to show up as a deep ache with horizontal extension, like reaching back for something behind you. None of these patterns exist in isolation. They’re entry points into a larger conversation about what the shoulder is actually doing.
The fix isn’t usually about the deltoid itself. Soft tissue work directly on the deltoid can provide relief, and there are times when that’s exactly what’s needed. But if the rotator cuff is still underperforming, if the scapula is still sitting in the wrong position, if the pectoralis minor is still short, the deltoid goes right back to compensating the moment the work stops. The assistant foreman can only cover for so long before the system needs the people above him to show up and do their jobs.
When the shoulder is working the way it’s supposed to, the deltoid moves the arm and the rotator cuff keeps everything honest underneath it. That’s the arrangement. The deltoid does the visible work. Everyone else makes the visible work possible.