Neighborhood 4 — Lower Back
The Bridge Builder
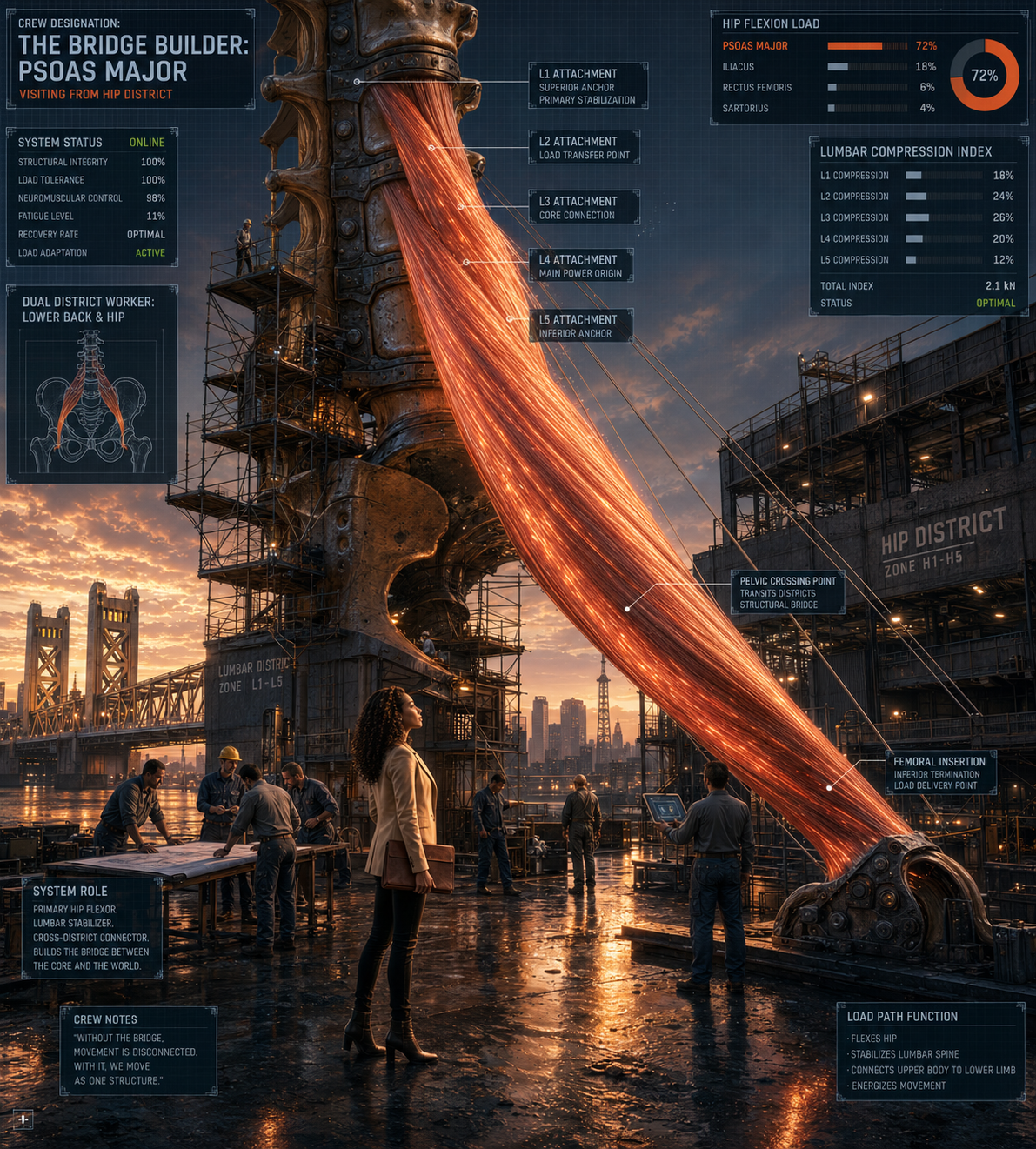
Worker 14 — Psoas Major — Visiting from Hip District
Note: This is the Lower Back District view of the Bridge Builder. The home district profile is in Neighborhood 5 — Hip District.
The psoas major is the only muscle in the body that connects the lumbar spine directly to the femur. It starts at the vertebral bodies and discs of T12 through L5 — the bottom of the thoracic spine all the way down through every lumbar segment — and runs diagonally through the pelvis to attach at the lesser trochanter on the inside of the upper thigh. No other structure does this. The psoas is the literal bridge between the spine above and the leg below, and when it’s in trouble, both neighborhoods feel it.
From the lower back district’s perspective, the psoas is a frequent and underappreciated contributor to lumbar problems. When the psoas shortens — which happens predictably in people who sit for long hours, who sleep in a fetal position, who have been compensating for pain in the hip or pelvis — it pulls the lumbar vertebrae forward and down. The lumbar curve increases. The discs at L4-L5 and L5-S1 load asymmetrically. The erector spinae brace hard to resist the forward pull. The quadratus lumborum compensates for the lateral instability that follows. The whole lower back neighborhood recruits harder than it should because one visiting worker has been pulling in the wrong direction for too long.
What makes the psoas unusual from a treatment standpoint is that it’s not a surface muscle. It lives deep inside the abdominal cavity, sandwiched between the spine and the abdominal organs. Direct access requires skill and appropriate technique. Most people trying to address their own psoas tightness through stretching are working around it rather than through it, and standard hip flexor stretches load the rectus femoris and iliacus more than they reach the psoas itself.
The most effective psoas release work combines direct soft tissue treatment of the muscle through the abdominal wall with contract-relax techniques that use the muscle’s own neurological pathways to reduce tone. Paired with addressing the downstream effects — the erector bracing, the QL compensation, the anterior pelvic tilt — the lower back typically responds in ways that purely lumbar treatment hasn’t been able to achieve.
The relationship between the psoas and the lower back is bidirectional. Lower back pain changes how the psoas loads. A tight psoas changes how the lower back loads. Treating one without the other is like fixing one end of a bridge while the other end stays broken. The bridge builder visits the lower back district regularly. Understanding what it’s bringing with it each time changes the way the lower back gets treated.