Neighborhood 5 — Hip District
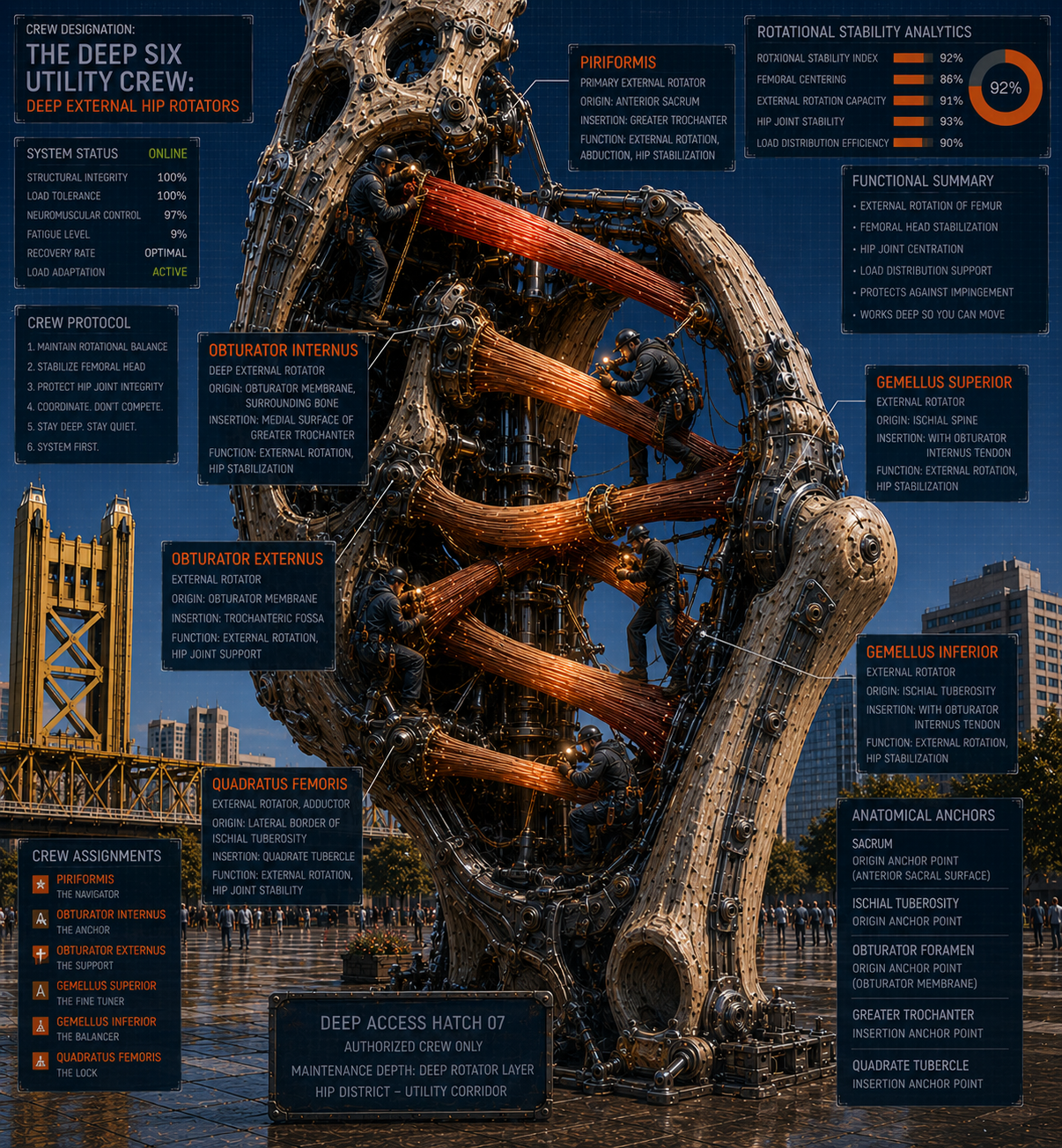
The Deep Six Utility Crew
Worker 17 — Deep External Hip Rotators
Six muscles live in the deep posterior hip — piriformis, obturator internus, obturator externus, gemellus superior, gemellus inferior, and quadratus femoris. Most people have heard of one of them: the piriformis, usually in the context of sciatica-like pain and the internet diagnosis of piriformis syndrome. The other five are largely unknown outside anatomy classrooms. But they function as a unit, and treating the piriformis in isolation while ignoring the rest of the crew is one of the reasons piriformis problems keep recurring instead of resolving.
The primary job of the deep six is external rotation of the hip — rotating the femur outward in the socket. They also assist with hip extension and, crucially, with stabilizing the femoral head in the acetabulum during movement. Think of them as the fine-positioning crew for the hip joint, making micro-adjustments to keep the ball sitting correctly in the socket every time the leg moves. When they’re working correctly, this is invisible. When they’re not, the hip socket loads asymmetrically, the piriformis clenches protectively, and everything downstream from the femur starts to work around the instability.
The sciatic nerve is the reason the piriformis gets so much attention. In most people, the sciatic nerve passes below the piriformis. In a significant percentage, it passes through or above it. A piriformis in spasm — which can happen when the deep hip rotators are generally overworked or compensating for weak glutes — compresses the nerve and produces pain, numbness, and tingling that travels down the back of the thigh and into the calf in a pattern that closely mimics lumbar disc herniation. Distinguishing between true sciatica from a disc problem and piriformis-mediated sciatic symptoms is important because the treatment is entirely different, and one of the most common reasons people end up in spine surgery that doesn’t fix their pain is because the piriformis was the actual source.
What causes the deep six to become dysfunctional is almost always the same story as the rest of the hip district: a weak gluteus maximus, a weak gluteus medius, and a pelvis that’s been sitting in anterior tilt long enough that the deep hip rotators have been chronically loaded in a shortened position. The piriformis and its colleagues end up substituting for the stability the glutes should be providing, and muscles in chronic contraction develop the pain sensitivity and referral patterns that send people looking for explanations they can’t find on an MRI.
Direct work on the deep six — carefully applied, with attention to the sciatic nerve’s position and the surrounding structures — can produce substantial relief from deep hip pain, SI joint pain, and sciatic-type symptoms. The piriformis responds particularly well to release through the glute tissue. The rest of the crew benefits from movement-based work that reestablishes external rotation control rather than just passive range. And the foundational work is, as always, getting the glutes to do their job so the utility crew can stop filling in for absent management.